Why is it so hard to move someone from a hospital bed to a care home?
Or “The case of Iris Sibley, who has been left stranded in Bristol Royal Infirmary for more than six months because a nursing home place could not be found for her.”
Spare a thought for Iris, who spent 6 months in Bristol Infirmary – even though she was ready to leave – because a nursing home bed could not be found for her.
CSI stands for Care Sector Innovations, but for this Insight I have changed it to "Crime Scene Investigations" – because what happened to poor Iris is a definite crime, not one punishable by law maybe, but one that must eradicate.
I am not trying to add to the national dailies who have all already reported this “scandal”. CSI is just investigating whether the delay was down to a shortage of beds in the area.
So what did Crime Scene Investigations find?
According to the Care Quality Commission (CQC) register, there are around 210,000 care home nursing beds in England – an average of 46 beds for every person aged 75 and over (who make up 90% of all residents). This supply level is enough to drive average occupancy levels of 90%, which is a sensible, if not ideal, level for care providers, as there is a capacity for people in need of a care home bed. Unfortunately this “average” supply level varies greatly across the country.
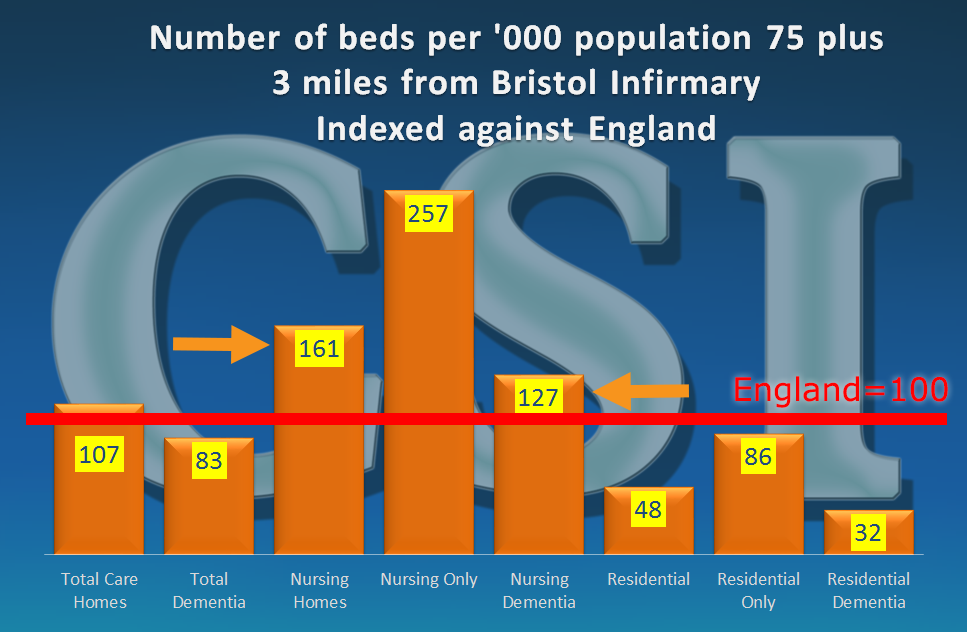
We looked at a 3 mile radius of Bristol Infirmary:
There are 19 care homes with nursing with a total of 1,260 beds
This works out at around 74 beds per ‘000 population, 61% higher than the national average
Nursing Dementia, the type of bed that Iris would have needed at the time, has supply levels around 27% higher than the England average.
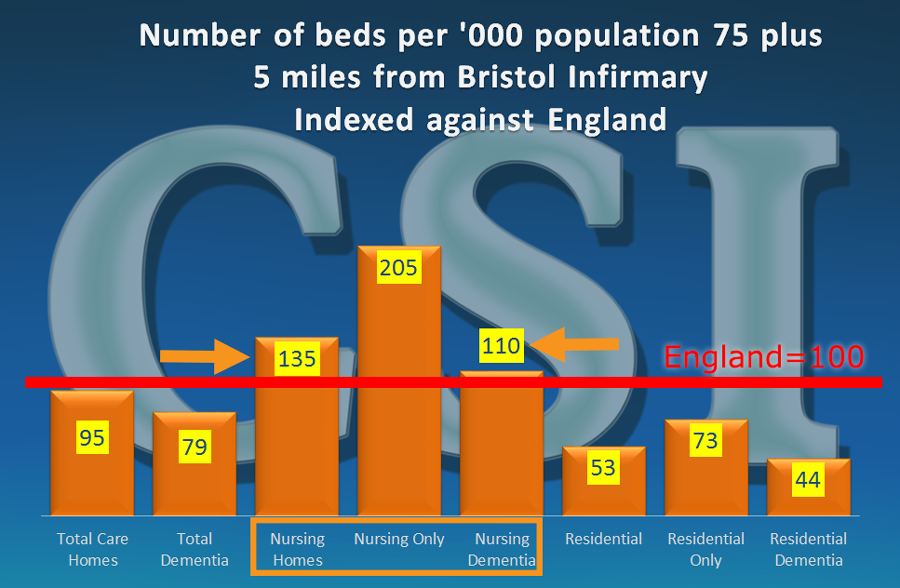
Then a 5 mile radius:
There are 37 care homes with nursing with a total of 2,268 beds
This work out at around 62 beds per ‘000 population, 35% higher than the national average.
Nursing Dementia, the type of bed that Iris would have ideally needed at the time – has supply levels around 10% higher than the England average.
In both cases we did also find that residential and residential dementia beds were under supplied, and so there maybe people living in homes with nursing, who would otherwise have been more suited to a residential home.
So, the local area has a higher supply level of nursing and nursing dementia beds than the national average. But if Bristol Infirmary took 6 months to find a suitable bed, what chance have other hospitals got where local supply is much lower?
There were other issues cited in this struggle, where a care home with vacancies was found, in a suitable location, but unfortunately, the quality of the home was not up to family requirements.
The CQC has rated about 66% of the nursing homes they inspected in the area as Good, 34% as Requiring Improvement – with no “Outstandings” or “Inadequates.” This is slightly better than the national average, so it wasn’t quality levels that were instrumental in the delays, any more than it would be in the rest of the country.
In February 2016 CSI reported on the massive variances in the local supply of care home beds across the country. Obviously if you have areas over relative oversupply in some areas there will be under supply in others. Only 32% of local authorities in England come within 5% of the national average supply level, with the highest level being 153 beds per ‘000, and the lowest only 26 per thousand.
And the 75 plus population continues to grow, against a net reduction of around 2,500 care home beds over the last 2 years. And reports suggest that many of the homes that are currently open are struggling to keep things that way.
So, the problem will get even worse if we cannot address this downward trend – we need new homes – and we need them in the right locations.
But back to the problem of releasing people from valuable hospital beds when they are ready to leave. It is important that NHS hospitals work closely with local authorities and care providers, to develop a contingency plan for future situations, which will continue and probably increase.
The process should become more proactive, rather than reactive.
If not currently doing so, the NHS and Local Authorities need to
Create a detailed database of local care providers, detailing specifically what types of care they can offer (e.g. nursing, residential, dementia, mental health) and alongside it,
Manage a “live” bed vacancy reporting system, so that whoever is trying to arrange a location, will have this information at their fingertips, and quickly identify a suitable location, and fast track the discharge and admission process before that bed is filled.
With this type of plan in place, they would undoubtedly have found Iris a bed much earlier.
But her son is reported as saying, when they did find a suitable home, whilst waiting for the NHS to authorise it, the vacancy disappeared. Whoever is charged with finding a suitable bed must be given the responsibility to sign it off immediately a suitable location has been found.
The whole care sector, (and the lawyers), are currently trying to understand and agree benchmarks for the “Deprivation of Liberties Safeguards” (an amendment to the 2005 Mental Health Act.) If this wasn’t a deprivation of Iris’s Liberty, what is?